Download leaflet
What is Tracheoesophageal Fistula (TOF)?
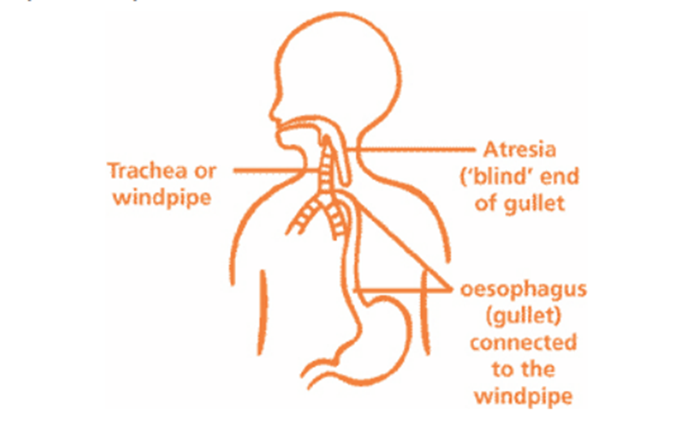
TOF is a condition in which a connection (fistula) forms between the oesophagus (the tube that leads from the throat to the stomach) and the trachea, or windpipe (the tube that leads from the throat to the lungs). Normally, the oesophagus and windpipe are not connected, and liquids swallowed by your baby go directly into the stomach.
What is Oesophageal Atresia (OA)?
OA happens when a gap forms in your baby’s oesophagus (food pipe). This means there is no continuous passage to the stomach and your baby’s milk cannot pass from his or her throat to the stomach. The blind end of the upper segment of the oesophagus will form a pouch like structure.
OA can occur without being associated with TOF but the incidence of them both occurring together is high. There are 4-5 different combinations of TOF/OA
Why does TOF/ OA Happen?
The exact cause of TOF/OA is not known and is not caused by anything you may or may not have done during pregnancy. It is thought to occur during your baby’s early development in the womb, though the reason for this is not understood. It occurs in one in 3500 to 5000 births. It is equal between males and females. The risk of occurring in subsequent pregnancies is less than 1%. It can happen on its own or be associated with other abnormalities of the heart/kidney/spine/limb/rectum etc.
How to Confirm TOF/OA
TOF/OA cannot always be diagnosed before birth. It maybe suspected on an antenatal scan if too much amniotic fluid is detected in the womb (Polyhydramnios) though there may be other causes for this. Usually TOF/OA is confirmed soon after birth. Your baby will present with breathing difficulties, drooling saliva from the mouth and nose. This is due to the blind pouch of the oesophagus (food pipe) filling with saliva and mucus, causing these secretions to back up into the mouth and nose.
To further help with the diagnosis, the midwife or team looking after your baby will try to pass a tube (Nasogastric tube) through your baby’s nose into the stomach. They will find that it will not pass into the stomach and an X-ray of the chest/stomach will confirm that the tube is coiled in the blind pouch confirming the diagnosis.
How can TOF/OA be Treated?
The definitive treatment for TOF/OA is surgery. However, the first line of treatment will be to stabilize your baby. This will mean your baby will need a special tube called a ‘Replogle’ tube. The tube will be passed through your baby’s nose or mouth and the tip of this tube will sit in the blind pouch of the esophagus. The other end of the tube will be attached to a low grade suction machine. This machine will continuously drain any saliva from pooling in the pouch thus reducing the risk of aspiration.
As your baby will be unable to feed, fluids will be given through a drip into their veins. Your baby’s breathing, heart rate and oxygen levels will be closely monitored. If any changes are observed in their condition, treatment will be initiated as required.
The surgical team will explain in more detail what the operation will involve and answer any questions/concerns you have. An anaesthetist will also visit you and discuss the anaesthetic procedure, risks and what pain relief will be best for your baby. Consent will be required from you before the operation can proceed.
Although your baby cannot have milk at this time if you are planning to breastfeed your baby later on by breast/bottle, you should try to start expressing breast milk within 6 hrs of birth. The nursing staff will be able to support you in how to use the breast pump to express your milk. Your milk will be stored in a freezer on the unit until such time the surgeon/neonatologist feels your baby is well enough to commence milk feed.
Surgery
To repair the TOF, the surgeon will separate the oesophagus from the trachea and repair the part of the trachea where the oesophagus was originally joined. The method to repair the OA depends on the distance between the two ends of the oesophagus. In most cases, the surgeons will cut the blind ends of the oesophagus and join the two ends together to form a continuous tube. At this time, the surgeons will insert a TAT (Transanastomotic tube), which is a flexible tube passed up one nostril down the oesophagus (Food pipe) into the stomach to use for feeding your baby later on.
In rare cases of ‘Long gap’ OA, where the distance between the 2 ends of the oesophagus is too wide to be joined straight away, different treatment will be required. In such scenario, a gastrostomy tube (a temporary tube inserted directly into the stomach by surgeon) is inserted into the stomach for your baby to have milk feeds whilst a decision is made for future operations and the timing of those.
If this is likely to be the situation, the surgeons will explain this to you. All doctors who perform this operation have had lots of experience and will minimise the chance of problems occurring.
Depending on the type of TOF/OA, some babies will need a higher level of care, which will be provided in the intensive care unit. Once this intense care is reduced your baby will be transferred back to the surgical neonatal unit where monitoring and close observations will continue.
Throughout your baby’s post operative recovery, his or her pain will be assessed and managed appropriately with analgesia (pain relief medication).
When it is time for your baby to feed, milk will initially be given via the TAT tube. In some situations, nutrition may be supplemented in a different way with Parenteral Nutrition (PN) via a drip. Introduction of oral feeds will be approximately after a week, and the surgeon will make this decision depending on the recovery of your baby. If any problems occur during oral feeds, further investigations will be required.
You may feel anxious, especially while your baby is connected to drips and monitors, but it will become easier with time. If you are worried about caring for your baby, please talk to the nurses.
Your baby will need to be seen again after they leave hospital to check on their progress, and you and your baby will be seen in the joint TOF and dietician clinic to monitor progress and weight. These appointments will be conducted regularly.
What Problems can Occur Following Surgery?
Feeding problems may occur due to the oesophagus narrowing where it was originally repaired. Sometimes it needs widening/stretched and this will require an operation at a suitable time after discussion with your surgeon.
Older children also complain of problems with swallowing and if needed your baby maybe referred to a speech and language therapist for further advice.
Your baby may have already commenced on some medicine for Gastro Oesophageal Reflux (GOR). This is where the contents of the stomach flow back up the oesophagus causing pain and irritation. GOR can be an ongoing problem.
When babies start to wean and textured food introduced, dietician input is necessary to introduce these foods safely.
At Home what to Watch Out for?
- More dribbling and drooling than usual.
- Breathless during feeding.
- Change in your baby’s colour during feeds i.e. blue.
- Difficulty when breast/bottle feeds.
- Coughing and choking when feeding.
- Has difficulty in swallowing saliva or feeds.
- If you observe these symptoms please get medical help immediately.
Contact:
If you have any concerns or worries about your baby once you are home you can call the Neonatal Surgical Unit and one of our Nurses will be happy to give you advice and reassurance.
Neonatal Unit 1C Yellow Pod
Tel:0151 252 5378
Other Useful Contacts 
TOFS
Website: https://tofs.org.uk
Email: [email protected]
Tel: 0115 961 3092
Please ask the staff for ‘The TOF Book’ if you are interested to know more about TOF.
This leaflet only gives general information. You must always discuss the individual treatment of your child with the appropriate member of staff. Do not rely on this leaflet alone for information about your child’s treatment.
This information can be made available in other languages and formats if requested.
Alder Hey Children’s NHS Foundation Trust
PIAG: 454