Download the leaflet
What is Exomphalos?
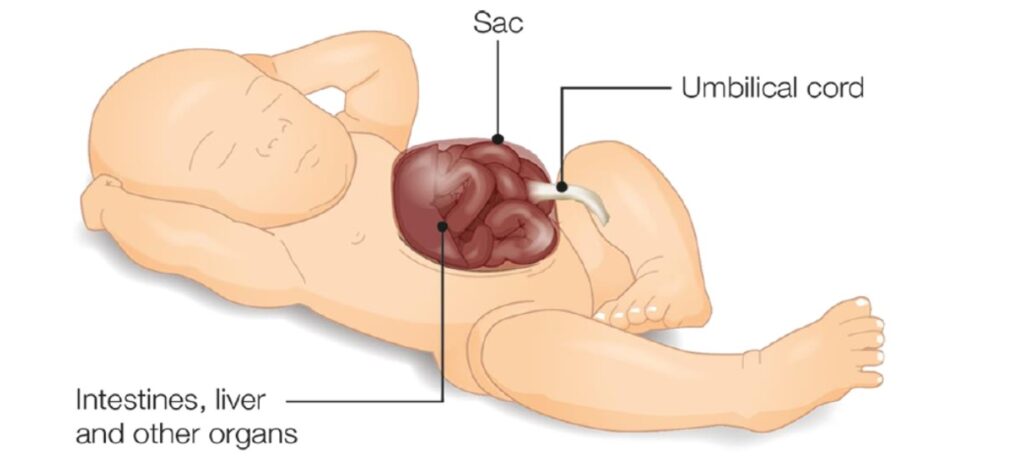
An exomphalos is a defect where your baby has a hernia or weakness in the abdominal wall at the umbilicus (tummy button). It is sometimes called an Omphalocele. Early in all pregnancies, the baby’s bowel develops inside the umbilical cord (belly button). It usually moves inside the abdomen a few weeks later. With an exomphalos, your baby’s tummy wall has not closed around the base of the umbilical cord meaning that some organs protrude outside the body. It is usually just the intestine (bowel), but sometimes the liver and other organs as well. The organs outside the abdomen are contained within protective sac, so it is like a balloon at the base of the umbilical cord.
The size of a baby’s exomphalos will depend on the number of organs contained within the sac on the outside of their abdomen. Smaller exomphalos is less than 5 cm and has only bowel inside it (Exomphalos minor) and exomphalos major has a larger size of more than 5cm and has liver inside the sac. Exomphalos affects around 1 in 8000 babies.
What causes Exomphalos?
We do not know what causes exomphalos. It is not caused by anything you may or may not have done during pregnancy. It is often linked to other medical conditions like those affecting your baby’s chromosomes (genetic information) or heart. You will be able to discuss your individual circumstances with the specialist team.
How is Exomphalos diagnosed?
Exomphalos can be diagnosed on antenatal scans and upon birth. The organs in a protective sac, which appear on the outer surface of the abdomen. This confirms the diagnosis.
How to treat Exomphalos
Once your baby is delivered, the neonatologists will see if your baby will need any help with breathing. It is usually the babies with a very large exomphalos that may need help with their breathing. The sac will be covered with moist dressings and placed in a plastic bag. This is to protect the exposed sac with moisture and warmth. We aim to make sure you can see and cuddle your baby before he or she is moved to the neonatal unit.
- To begin with, your baby will be nursed in an incubator and will have a nasogastric (NG) tube passed through his or her nose into the stomach. This will drain off the contents of the stomach and stop your baby feeling and being sick. It also releases any excessive air from the stomach, which could make your baby uncomfortable. He or she will also have an intravenous infusion (drip) of fluids.
- Your baby should then be safe and stable and can be transferred to a surgical unit at a convenient time. Although your baby cannot take milk at this time, if you plan to feed your baby breast milk later on (either by breast-feeding or by bottle) you should start expressing breast milk within 6 hours of birth. Feeds will be started depending on the surgical team. The nursing staff on the unit where your baby is will be able to show you how to express and store your milk and arrange for you to have access to a breast pump. Providing breast milk for your baby supports in overcoming the challenges they face whilst in intensive and special care.
Surgery
Small exomphalos: To repair the small exomphalos, an operation will be necessary under general anaesthetic. The surgeons will move the intestines back inside the abdomen and then close up the muscles and skin, making a belly button at the same time.
Large exomphalos: if the defect is large, it might not be possible to repair it soon after birth. In these cases the sac will be protected with protective dressings, the baby will be allowed to feed and grow. Your baby will be regularly assessed for their growth, strength of the sac and reduction of the bowel and organs into the abdominal cavity. An operation will then be planned electively.
Are there risks with surgery?
The surgeon will explain about the operation in more detail, discuss any worries you may have and ask you to sign a form giving consent for your child to have the operation. An anaesthetist will also visit you to explain about the anaesthetic and discuss pain relief for your baby.
All the doctors who perform this operation have had lots of experience and will minimise the chance of problems occurring. It can take a while after the operation for the bowel to start working properly so your baby may need to be fed intravenously using parenteral nutrition (PN) for a while. Some babies with exomphalos may have breathing problems, which will require more support for a longer period.
What happens after the operation?
Your baby will come back to the ward in the incubator to recover, and you will be able to visit as soon as he or she is back on the unit. All babies are closely monitored after the operation, and so your baby will be connected to monitors to check his or her breathing, heart rate and oxygen levels. He or she will also be given pain relief through the intravenous infusion (drip).
While your baby’s intestines recover and start to work, he or she will be fed through a tube into his or her veins (this is known as parenteral nutrition or PN). Your baby may have mouth care with breast milk even though milk is not been given as feed. The PN will gradually be replaced by milk, given through the naso-gastric tube when your child is able to tolerate this.
As your baby recovers, you will be able to feed him or her by mouth, ideally from the breast. Overtime, the drips and monitors will be removed one by one. The nurses on the ward will encourage you to look after your baby and support you along the way.
You may feel anxious, especially while your baby is connected to drips and monitors, but it will become easier with time. If you are worried about caring for your baby, please talk to the nurses. You will be able to go home or be transferred back to your local hospital once your baby is feeding properly and gaining weight. Your local health visitor or community paediatric nurse will visit you regularly. Your baby will need to be seen again by the surgeon after discharge to check that everything is okay, and a letter will be sent out to you in the post to tell you when the clinic appointment will be.
How long will your baby stay in the Neonatal Unit?
The length of your baby’s stay in hospital will depend on:
- Once the surgical team feel dressings for larger exomphalos can be carried out on an outpatient basis.
- Whether they have any other medical conditions.
- Whether they were born early.
What is the outlook?
The outlook for baby’s with exomphalos varies, depending on the size of the defect and any other problems. Sometimes it takes a while for your baby’s intestine to work properly, so your baby may need extra nutrition. This could involve special feeds or continuing PN for a longer period.
Contact
If you have any concerns or worries about your baby once you are home you can call the Neonatal Surgical Unit and one of our Nurses will be happy to give you advice and reassurance.
Neonatal Unit 1C Yellow Pod
Tel:0151 252 5378
Other Useful Contacts
GEEPS (Gastroschisis, Exomphalos and Exstrophies Parents Support)
GEEPS can offer help and support.
Website: www.geeps.org
This leaflet only gives general information. You must always discuss the individual treatment of your child with the appropriate member of staff. Do not rely on this leaflet alone for information about your child’s treatment.
This information can be made available in other languages and formats if requested.
Alder Hey Children’s NHS Foundation Trust
PIAG: 456