Department of Surgery
Information for parents and carers
Download leaflet
Spinal Scoliosis Information for Parents and Carers PIAG 38 (304kB)
What is Spinal Scoliosis?
Scoliosis is a change in the shape of the spinal column. The spine can curve and twist. This may lead to changes in the shape of the ribcage or the waist.
There are three main causes for a curve;
- Congenital (present at birth).
- Neuromuscular, (caused by a condition like cerebral palsy or muscular dystrophy).
- Idiopathic (the cause is unknown).
In 80% of cases, the cause is unknown.
Why is surgery needed?
An operation is often required for patients who have a large curvature of the spine or one which is likely to worsen.
The purpose of surgery is to partly straighten the spine, improve the shape and prevent the curve from deteriorating by encouraging selected bones of the spine to heal together (a fusion). If your child is in a wheelchair, the changes in the spine and pelvis may have made seating more difficult, with a tendency for your child to lean to one side. The aim of surgery is to give the spine a better position.
What does spinal surgery involve?
There are two main types of spinal surgery;
Anterior surgery: an incision (cut) is made at the side of the patient’s ribs.
Posterior surgery: an incision is made on the patients back.
Costoplasty: a removal of a section of ribs.
Your child may require one or more approaches to the surgery; you will discuss this with their Spinal Consultant. Your child will be in theatre between six and nine hours and will have a general anaesthetic (be asleep).
During surgery, numerous screws are placed in the spine to gain an anchor. These are attached to rods which will hold the spine in the desired shape. The selected bones will heal together over time.
In younger children, a growth rod may be inserted instead to allow the spine to grow as the child grows. At later dates, smaller operations or procedures may be needed to lengthen the growth rod. A final operation will be performed when growth is complete to allow a compete fusion (joining of the bones) of the spine.
Surgery does carry possible complications; you will be given informed advice regarding these by your consultant before surgery. bones) of the spine.
Surgery does carry possible complications; you will be given informed advice regarding these by your consultant before surgery.
Will I need specialist equipment to care for my child?
Mobility and moving and handling equipment including, wheelchairs and hoisting for patients with neuromuscular conditions will be reviewed at pre-operative assessment by the nurse specialist and therapists.
Parents/guardians of patients should bring a contact list of the team members involved in your child’s care to the appointments. We will liaise with agencies to try and obtain suitable equipment for your child’s discharge. It is useful if you also keep local services involved in caring for your child updated.
If your child does not use any mobility aids, then no specialist equipment will usually be required for discharge.
Pre-admission information
Tests will be completed four to six weeks before surgery when you will see the spinal nurse specialist.
If your child is listed for correction of scoliosis, investigations and procedures will be completed including:
- X-rays.
- Lung function tests (a blowing test called spirometry).
- Electrocardiogram (sticky pads on the chest to monitor the heart called an ECG).
- Echocardiography (an ultrasound of the heart called an ECHO).
- Blood tests (using topical anaesthetic cream to numb the skin).
- Clinical photography.
- Clinical measuring.
If your child is frightened or has phobias please let us know ahead of this appointment and we will aim to provide additional support. We have specialist play therapists that can assist your child in their hospital journey.
Please be aware that this is a long day.
Idiopathic Scoliosis patients will meet their anaesthetist on admission unless there is a clinical need for them to be reviewed earlier.
Neuromuscular patients (e.g. cerebral palsy, muscular dystrophy) will be reviewed by a spinal consultant anaesthetist, they will also see an Occupational Therapist to assess whether additional equipment is needed after surgery, this will be done at additional out-patient appointments.
The nurse specialist will first assess and order your child’s tests. Once completed the spinal consultant anaesthetist will review your child and their test results. They will discuss the anaesthetic and the potential risks/complications with you and assess your child’s suitability for surgery. A further appointment may be arranged if the anaesthetist requires discussions with other professionals or more investigations to be completed.
Please bring a list of any medications your child is taking to the pre-operative assessment and discuss with the team.
Certain types of medicines need to be stopped for clinical reasons, including the combined oral contraceptive pill and certain anti-coagulant therapies up to six weeks before surgery.
Young people who smoke will have their operation cancelled. The Trust can provide information and advice to young people who need help to stop smoking.
If your child develops a cold, has an infection or is unwell before their admission please let us know. Please contact us on the numbers listed at the end of this guide.s listed at the end of this guide.
Things to consider before admission
It may be helpful for you to inform any professional involved in your child’s care/schooling of the surgery to allow them to plan for your child’s recovery.
If your child is regularly constipated, ensure they have had a bowel movement before admission using their usual prescribed laxatives.
You may wish to plan a visit to the hairdressers or barbers for your child before their surgery.
Growth can occur after surgery.
What to bring along for admission
Patients may bring in nightwear, but no onesies please. Comfortable, loose clothing for discharge.
Toiletries.
Please bring your child’s regular medications.
If hoists are used please bring slings.
Patients on non-invasive ventilation please bring along your equipment and or cough assist.
You may bring along feeds for gastrostomy fed children, the trust offers feeds for patients and will provide the pump and equipment.
Female patients are advised to bring sanitary protection into hospital.
You may bring along laptops/games etc. Please inform staff when you wish to charge any batteries to avoid fire hazards.
Ward Information
There will be a bed next to your child’s bed on the ward for one parent/legal guardian to stay. If your child is admitted to Intensive Care or High Dependency Unit, a parent bed will not be available but a comfortable chair is provided for a parent to stay.
There is a room on the ward for parents to have a drink, snack and freshen up.
No hot drinks on any of our wards please.
Express any specific dietary requirement to staff on admission.
Internet is available in some areas of the hospital.
Hospital teaching staff may attend to carry out some schoolwork.
Visiting times are open for Parents and Carers. Please check for visiting times on the ward for others wishing to come along. Parents and guardians are permitted to be with their children throughout the day and one may stay at night.
Ronald Macdonald House
This is a charity based on the Alder Hey site that offers parent accommodation. Unfortunately, rooms cannot be booked in advance and allocation of rooms is at the discretion of Ronald McDonald staff and will depend on availability.
Please inform staff on admission if you require a room. There are single rooms and family rooms they can provide travel cots etc.
If a room is not available, you may still use their cooking and clothes washing facilities.
They sell a range of items should you leave anything at home.
Please contact Ronald Macdonald House for more information if you wish, on the number listed later in this guide.
Parking and Travel
Discounted parking tickets are available from Concierge. This is on the ground floor of the hospital.
Please bring along documentation of any benefits you receive and travel receipts to produce at the Cash Office, should you wish to claim expenses.
Admission for surgery
If your child is having growing rods inserted for the first time or a definitive fusion for scoliosis correction, they will be admitted the day before surgery.
The ward you will be admitted onto will be 4A, this is the spinal orthopaedic and Neurosurgery ward.
You will be greeted by a member of the nursing team who will provide and apply hospital identification bands for patients. These should be worn throughout the entire stay.
Prior to surgery, a spinal surgeon will visit and explain the procedure again in detail and answer any further questions you may have. A parent / guardian or child over the age of 16 will be asked to sign consent confirming the operation.
A doctor from the anaesthetic team will visit. You may take this opportunity to discuss in detail the anaesthetic procedure, post-operative pain relief and address any concerns you may have.
A further blood test will be taken on admission / pregnancy test (urine test) for girls over 12 years.
Your child will be given pain relieving medication the night before surgery.
The operation day
Your child will be fasted (no food or drinks) before the general anaesthetic.
A tablet or medicine (pre-med) to help your child to feel relaxed will be offered the morning of surgery.
Patients with long hair are encouraged to wear loose braids.
A hospital gown will be provided for patients to be worn for theatre.
Local anaesthetic cream will be applied to your child’s hands to numb the skin for the anaesthetist to position the cannula (drip).
Both parents can accompany your child to the theatre corridor. One parent will be invited into the anaesthetic room. The anaesthetist will put a cannula in the back of your child’s hand and get them ready for surgery.
Once your child is asleep, a nurse will accompany you back to the ward.
Your child will be in theatre usually between six to nine hours or possibly longer. You may stay on the ward or go out. Please let the staff know if you are leaving the ward so they are able to contact you.
Your child’s spinal cord will be monitored by a specialist throughout the operation.
Blood transfusion may be necessary during or immediately after surgery. Bleeding is not unusual with spinal surgery. It can be necessary to replace the amount of blood a child has lost. Any blood lost during surgery is washed, filtered and given back to your child using specialist equipment (Cell Salvage).
Once woken from the anaesthetic, your child will be taken from theatre to the recovery area.
What to expect immediately after surgery
When your child is ready to be returned to the ward you will be invited to the recovery area to collect them with a nurse.
Occasionally admission to Paediatric Intensive Care Unit or High Dependence Unit may be required. Parents/guardians will be invited to be with patients.
Your child will receive intravenous fluids through several drip sites and pain relief which will be continued over the next few days, and a urinary catheter is inserted in theatre which will remain in place for a few days.
They may have a small tube left in the wound to drain small amounts of blood. They may have a chest drain if additional back and side approaches are necessary. Both of these drains are normally removed by 48-72 hours after surgery.
Please remember all these things are applied in theatre when your child is fast asleep and are easily removed afterwards.
Additional oxygen will be given, through a mask or tubes that sit under the nose and patients will be closely monitored on the ward.
As your child has been on their stomach throughout the operation their face or lips may be a little swollen, this will usually settle after a few days.
Patients may notice tiny scabs on their head, feet, arms and legs; this will be from the spinal cord monitoring.
Female patients may experience menstruation (a period).
What to expect immediately after surgery
When your child is ready to be returned to the ward you will be invited to the recovery area to collect them with a nurse.
Occasionally admission to Paediatric Intensive Care Unit or High Dependence Unit may be required. Parents/guardians will be invited to be with patients.
Your child will receive intravenous fluids through several drip sites and pain relief which will be continued over the next few days, and a urinary catheter is inserted in theatre which will remain in place for a few days.
They may have a small tube left in the wound to drain small amounts of blood. They may have a chest drain if additional back and side approaches are necessary. Both of these drains are normally removed by 48-72 hours after surgery.
Please remember all these things are applied in theatre when your child is fast asleep and are easily removed afterwards.
Additional oxygen will be given, through a mask or tubes that sit under the nose and patients will be closely monitored on the ward.
As your child has been on their stomach throughout the operation their face or lips may be a little swollen, this will usually settle after a few days.
Patients may notice tiny scabs on their head, feet, arms and legs; this will be from the spinal cord monitoring.
Female patients may experience menstruation (a period).
Pain relief following surgery
Spinal surgery is a big operation and it may not be possible to take away all of the pain in the early days after surgery. Medication will help, and your child should be more comfortable as they begin to recover. Please be aware that they are unlikely to be completely pain free during the first few days / weeks after their operation.
The Acute Pain Team (a specialist group of doctors and nurses experienced in pain management), will be actively involved in your child’s care plan.
Wherever possible, your child will be encouraged to use pain scores. Please see an example of our charts later on in this booklet.
Pain relief is mainly provided through a combination of strong pain medications given through a drip into your child’s vein (intravenous) and orally (by mouth). Please note that oral medication can be administered through a gastrostomy site, when appropriate.
Occasionally, additional pain relief in the form of a pleural catheter (a small tube inserted into the chest) is provided through which local anaesthetic can be given. This will temporarily block pain signals in the nerves and provide temporary numbness.
Generally four or five days after surgery, all intravenous analgesia (pain relief) will have been stopped and your child will be transferred onto regular oral medication or receive medication via their gastrostomy site.
Post-operative recovery
If your child has had posterior (incision at the back) surgery, they will probably be able to have a drink by the next morning. If they tolerate oral fluids without being sick, then they will be offered something light to eat.
Antibiotics will be given for 48 hours after surgery to help prevent infection.
Your child will also be given regular laxatives to prevent constipation which is common after having major surgery and taking pain relief. If patients experience regular constipation please let the team know.
Some patients may experience itchiness which can be a side effect of the pain relieving medication, if this happens, they can be prescribed antihistamine.
Your child will be re-positioned regularly, and encouraged to move around gently as soon as they are able. As part of your child’s recovery nursing staff will be encouraging them to do breathing exercises. Our aim is to get patients out of bed the day following surgery.
Blood will be taken in the first few days after surgery to check iron levels. Your child may occasionally need a blood transfusion, or a course of iron which is taken orally.
As your child gets better, the intravenous fluid lines, drains and urinary catheter will also be removed and these are usually pain free procedures.
The nursing team will encourage mobility and will assist your child to sit in a chair. If they can do this comfortably, then they will assist them to walk. If your child usually climbs stairs, physiotherapists will assess them on our stairs and ensure that they can go up and down stairs before they go home.
If your child has a neuromuscular condition your usual moving and handling techniques may need to be modified after surgery. Nurses, physiotherapists and an occupational therapist will encourage hoisting and sitting out for short periods of time to begin with and build these times up during your stay, to ensure a good seating position before discharge.
Sometimes patients may need to be fitted with a temporary brace and this will be made and fitted by the hospital Orthotic technician (an Orthotic technician makes external devices to help with specific conditions) before discharge. Please ask your consultant how long you may have to wear this.
Going home
Patients can usually be discharged between four to ten days after surgery, although this will depend on their type of surgery, and how they feel. An X-ray will be taken before discharge to check the position of the metalwork inserted during surgery.
Your child will be able to go home in your own transport.
If you do not have transport, inform ward staff on admission and the hospital will provide an ambulance for the journey home.
For children with neuromuscular scoliosis that have an established nursing respite centre, a short stay may be very useful to ease the transition home.
Caring for your child at home after surgery
Being in hospital can disrupt a child’s normal day-to-day routine, it can take some time to get back to normal. Encourage them to be as active as possible, but expect them to feel more tired than usual.
Patients will be given pain relieving medicines to take home on discharge. They should continue to take these regularly for the first two weeks. Regular pain relief may be necessary for four to six weeks.
Continue to re-position your child regularly and encourage mobility. If you lift your child, make sure that you support them under the buttocks and around the back. Avoid lifting your child under the arms. If your child normally uses a wheelchair, you may need to use a hoist to lift them in and out of the chair. If a spinal brace is required for a time post operatively this should be applied before hoisting.
Returning to usual activities
For previously well children, we would anticipate your child will be mobilising, eating and drinking a well-balanced diet, and be able to resume some of their activities of daily living.
The wound should be healing without any complications.
Your child may take a shower as soon as they are mobile. If the dressing gets wet it should be changed immediately. The ward will provide some spare dressings, if you require more please contact your GP.
Patients are asked to wait four to six weeks after surgery before taking a bath to ensure wound healing.
For children with more complex needs, our expectation for discharge is much the same, although the recuperation may take longer.
On average a six week break from education is taken.
Commonly asked questions
- Can I still have children?
Yes spinal surgery will not stop you from having children. Always inform your maternity provider if you have metal work in your spine in case of epidural requirements.
- Will I have a scar?
Yes, unfortunately spinal surgery is not a scar free procedure.
- Will I set alarms off at airports?
Possibly, but you do not need to take any evidence of your surgery with you. Many people set alarms off at airports and the staff will use normal security protocols should this occur.
- Do I need to tell my insurance provider if I travel?
Always inform your healthcare insurance provider of pre-existing medical conditions and if metal work is in situ.
Follow-up arrangements
A wound check will be organised by ward staff for one week after discharge Please ensure that until the wound is healed it does not get wet. Once the scar has healed, please keep it out of the sun until it is no longer pink. Always use total sun block or clothing.
The specialist nurse for infection surveillance will contact you after discharge to ensure the wound / scar has healed and there has been no infection. If you notice any redness, swelling, oozing, pain or tenderness at the operation site, please contact us for advice using the numbers listed at the end of this guide.
Three months after your child’s surgery, an out-patient review with a spinal consultant will be organised. X rays and clinical photography will take place that day.
Patients will have a further two appointments with their consultant / nurse specialist, and be followed up for two years after surgery.
Contact details
Name: Lisa Andre, Emily Grant, Suzanna Reyes Spinal Nurse Specialists
Tel: 0151 282 4679
Email: [email protected]
Name: Sheila McKenzie, Spinal Team Pathway Co-ordinator for Mr Davidson / Mr Jayesh Trivedi Neil
Tel: 0151-252 5923
Email: [email protected]
Name: Lauren Craney, Spinal PCO to Mr Sudarshan Munigangaiah / Mr Marcus DeMatas
Tel: 0151 252 5912
Email: [email protected]
Name: Karen Day, Spinal PCO to Mr Dheerendra
Tel: 0151 252 5376
Email: [email protected]
Name: Charlotte Chamberlain, Spinal PCO to Mr Mohammed
Tel: 0151 282 4680
Email: [email protected]
Ward 4A Weekend and evenings
Tel: 0151 228 4811 ex 3109
Orthotics (Appliances):
Tel: 0151 252 5318
Ronald McDonald House:
Tel: 0151 252 5869
Patient Advice & Advocacy:
Tel: 0151 252 5161
Activities following spinal correction
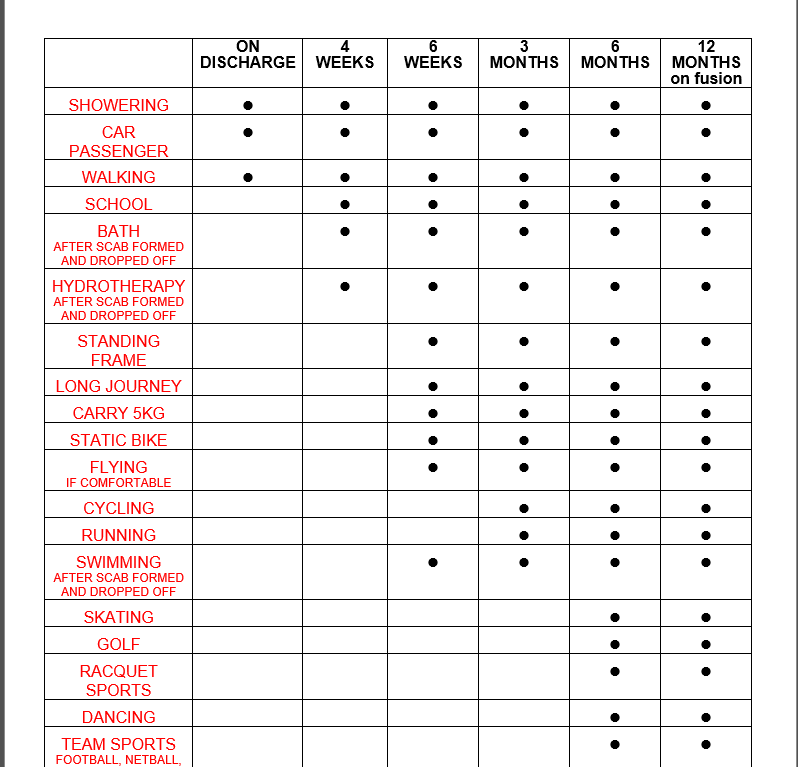
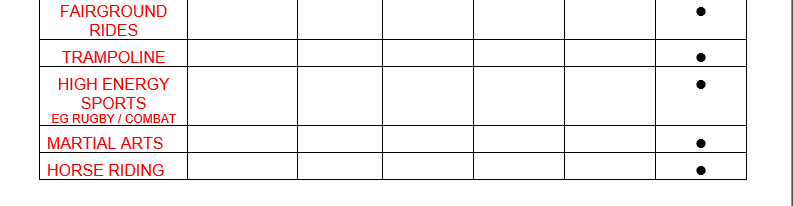
This leaflet only gives general information. You must always discuss the individual treatment of your child with the appropriate member of staff. Do not rely on this leaflet alone for information about your child’s treatment.
This information can be made available in other languages and formats if requested.
Alder Hey Children’s NHS Foundation Trust
Eaton Road
Liverpool
L12 2AP
PIAG: 38